[vc_row][vc_column][vc_column_text]I’m excited for Dec 21st. It’s the winter solstice, and it’s just 5 days away. That means the days will start to get longer! Here in the Pacific Northwest, winter hits me hard; the rain and the shorter days have a significant impact on my overall well being, and my mental health as a result. This seasonality of feeling down is often called the winter blues, or clinically diagnosed as Seasonal Affective Disorder (SAD).
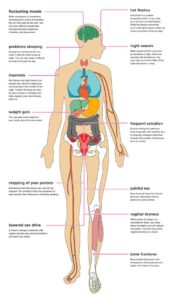
Characteristics of SAD are: sadness, anxiety, fatigue, difficulty concentrating, loss of interest in usual hobbies or activities, and sleeping more.
It has taken a while to learn how to manage this yearly change with the help of my doctors and naturopaths, and honestly it still sneaks up on me even with how much I know. Here are a few things I have learned to manage the winter blues.
(Please consult your primary care physician if you suffer from these symptoms, support goes a long way in managing SAD or any mental health condition)
Vitamin D
Get your levels tested. The journal Nutrition Research states that about 42% of U.S. adults are deficient in this nutrient . Vitamin D can be found in a variety of foods such as oatmeal, mushrooms, tuna, salmon, and milk. According to Yale Medicine, Vitamin D is manufactured in the skin when exposed to sunlight. Hence why shorter days in the northern latitudes this time of year results in more individuals impacted by this deficiency, oh and it’s cold so all our skin is covered up! Supplementation is often the recommendation for this deficiency. Vitamin D helps in calcium absorption, immune function, regulating neuromuscular system, and healthy cell cycles.
Go outside

This is one of the most powerful pieces to the puzzle! Yes, it’s raining here in Oregon, but a raincoat and a waterproof pair of shoes make all the difference. Getting your heart rate up and being outside during daylight hours helps to regulate your circadian rhythm, which tells your body when it should sleep.
Without sun exposure, our bodies naturally have a circadian rhythm around 24 hrs 20+/- min (combined sleep and wake cycles), that means if you are not regularly exposed to bright light (the sun), that cycle can shift up to 1-2 hrs in a week, and 5-6 hrs in a month. As a result, this change to your biological clock can also impact your mood and hormones. One such hormone is Serotonin, which increases with sunlight exposure. This hormone helps with mood stabilization, and communication between nerve cells, to name just a few functions.
Life application
Exposure to sunlight is most impactful in the mornings when there is light to enhance optic flow to increase alertness through special photoreceptors in the eyes that relay subconscious light intensity to the brain (See Huberman Lab podcast). If regular daily sun exposure is not possible, taking 1 hr each weekend in the AM hrs can help to reset the shift that naturally happens throughout the week. But what about rainy days? Even on rainy days, the sun exposure through the clouds is higher than most of us assume; instead of 15 min on a sunny day, perhaps 30-45 min would be the required time outside on rainy or dreary days.
Happy lamps or Light therapy boxes
 These 10,000+ lumen light boxes/lamps help to convince your brain into thinking the sun is up and shining on those days when getting outside isn’t possible, or for individuals who work night and swing shifts. The intensity mimics the sun and regulates circadian rhythms (see above paragraph). It is typically recommended to use within 30 minutes of waking for 15-30+ min and no less than 2 hrs before bed time to regulate your circadian rhythms, which improves sleep quality, and hormone regulation. An individual needs to be facing the light, but please don’t look directly at it.
These 10,000+ lumen light boxes/lamps help to convince your brain into thinking the sun is up and shining on those days when getting outside isn’t possible, or for individuals who work night and swing shifts. The intensity mimics the sun and regulates circadian rhythms (see above paragraph). It is typically recommended to use within 30 minutes of waking for 15-30+ min and no less than 2 hrs before bed time to regulate your circadian rhythms, which improves sleep quality, and hormone regulation. An individual needs to be facing the light, but please don’t look directly at it.
Which to choose
There are a variety of choices for these lamps, from table top, floor, or even portable travel options. It all depends on your needs. I have two, one that sits on my breakfast table, and one for travel which I intend to bring to work with me for days like today, when it’s dreary and dark. Brands- When I got my Happy lamp years ago, there were not as many options and Carex was one of the few that was easily accessible via Amazon. Since purchasing my first light, I also looked into Circadian Optics travel light for use at work. The key is to find a lamp that is 10,000 lumens, a unit of light measurement; after that you can prioritize how compact, or maybe how aesthetically pleasing it is. (see The Depression Cure, for more information on happy lamp use)
5-HTP
It’s a precursor and building block to Serotonin, that awesome hormone that functions as a mood stabilizer and increases with sun exposure. A study in 2016 by Jacobsen et al, suggests that slow release 5-HTP is an effective adjunct in treatment of depression. Remember, more is not always better, low doses can have a significant impact. Many prescription anti-depressants work by increasing extracellular 5-HT (which studies show can be elevated by 5-HTP as well, Jacobsen 2016).
As with any supplement, please consult with your primary care physician first, especially if you are on any antidepressants or prescription medications.
Find a new Hobby
 I always try something new each winter, this year it’s weaving and maybe cross country skiing. It helps my brain to work with bright, stimulating colors, and to make something beautiful. Many of us naturally did something like this when stuck at home due to Covid restrictions and battling feelings of sadness and anxiety; some took up yoga, made sourdough bread, learned to crochet, or speak a new language.
I always try something new each winter, this year it’s weaving and maybe cross country skiing. It helps my brain to work with bright, stimulating colors, and to make something beautiful. Many of us naturally did something like this when stuck at home due to Covid restrictions and battling feelings of sadness and anxiety; some took up yoga, made sourdough bread, learned to crochet, or speak a new language.
Science supports the importance of hobbies
A new skill engages the brain and creates new neural pathways. Studies have shown that doing hobbies and activities we enjoy releases neurotransmitters, like dopamine, an important chemical that helps us feel pleasure and joy. No matter how small, hobbies provide us with the opportunity to feel a sense of accomplishment. As a result the brain releases neurotransmitters that stimulate positive pathways. In fact, some physicians are now prescribing people to try a new hobby that is not health or fitness related, purely for the joy and burst of dopamine it provides as a way to combat mild to moderate depression. (See The Science behind Hobbies)
Photobiomodulation
 It’s a big word, but studies of depression and low level light therapy which is a combination of red and infrared light, shows significant promise with being a successful treatment to combat many forms of depression. Schiffer et al. in 2009 found that after one treatment to the right forehead, there was a statistically significant reduction in patients HAM-D score even 2 weeks after their first and only treatment. (HAM-D is a clinician administered depression scale.)
It’s a big word, but studies of depression and low level light therapy which is a combination of red and infrared light, shows significant promise with being a successful treatment to combat many forms of depression. Schiffer et al. in 2009 found that after one treatment to the right forehead, there was a statistically significant reduction in patients HAM-D score even 2 weeks after their first and only treatment. (HAM-D is a clinician administered depression scale.)
While treatment to the forehead results in measurable changes in depression in this study, studies have shown occipital penetration of photobiomodulation is >11%, compared to ~2% for frontal bone (Jagdeo et al. 2012). The research is not as comprehensive surrounding transcranial photobiomodulation, however a handful of studies demonstrate significant promise with stroke, TBI, dementia, parkinsons, depression, and cognitive enhancement.
This is an exciting time to be looking into non-pharmaceutical ways to improve SAD and chronic depression. (Attend our upcoming Photobiomodulation Webinar to learn more about all ways it can improve your life, put on by Ian McVay PTA: IPA Physio Portland in January 2022)
Closing thoughts on Getting Started
There is no quick fix or one solution to the winter blues, as with most things in life it is a complex interaction within the body, which will require a multifaceted approach to improve SAD symptoms. Rather than one large change, perhaps pick a few small areas to work on to see the best long term results. Drink your morning coffee in front of a happy lamp, sign up for a zoom course on a new hobby you are interested in, take a walk or go outside for 15 min at lunch, and overall just be creative with how you integrate new habits into your life.
Good luck! Maybe we will pass each other on the trails in Forest Park this winter, pausing in the sunlight to increase optic flow, alertness, and serotonin.

Sources:
Forrest, K. Y. Z. , Stuhldreher, W. (2010). Prevalence and correlates of vitamin D deficiency in US adults. Nutrition Research, Volume 31, Issue 1, January 2011, Pages 48-54
Huberman, A. (Host). (2021, Oct 25). Timing Light, Food, & Exercise for Better Sleep, Energy & Mood (No. 43). [Audio Podcast Episode]. In Huberman Lab. https://hubermanlab.com/dr-samer-hattar-timing-light-food-exercise-for-better-sleep-energy-mood/
Hamblin, M. R. (2016). Shining light on the head: Photobiomodulation for brain disorders. BBA clinical, 6, 113–124. https://doi.org/10.1016/j.bbacli.2016.09.002
Ilardi, S., 2019. The Depression Cure: The 6-step program to beat depression without drugs. [Place of publication not identified]: VERMILION.
Jagdeo, J. R., Adams, L. E., Brody, N. I., & Siegel, D. M. (2012). Transcranial red and near infrared light transmission in a cadaveric model. PloS one, 7(10), e47460. https://doi.org/10.1371/journal.pone.0047460
McCabe, C. (2021, February 14). The science behind why hobbies can improve our mental health. Neuroscience News. Retrieved December 8, 2021, from https://neurosciencenews.com/hobby-mental-health-17765/.
Moriarty, C. (2018). Vitamin D Myths “D”-bunked. Yale Medicine, https://www.yalemedicine.org/news/vitamin-d-myths-debunked
Schiffer, F., Johnston, A. L., Ravichandran, C., Polcari, A., Teicher, M. H., Webb, R. H., & Hamblin, M. R. (2009). Psychological benefits 2 and 4 weeks after a single treatment with near infrared light to the forehead: a pilot study of 10 patients with major depression and anxiety. Behavioral and brain functions : BBF, 5, 46. https://doi.org/10.1186/1744-9081-5-46[/vc_column_text][/vc_column][/vc_row]













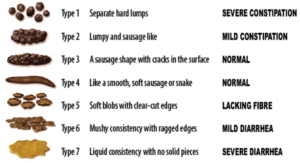
 –Poor diet — Be sure to check that fiber intake! Aim for 25-30g of fiber each day. Think pears, avocados, strawberries, oats, lentils, chickpeas, kidney beans, almonds, chia seeds, kale, spinach, etc.
–Poor diet — Be sure to check that fiber intake! Aim for 25-30g of fiber each day. Think pears, avocados, strawberries, oats, lentils, chickpeas, kidney beans, almonds, chia seeds, kale, spinach, etc. –
–  –
–  –
–