The Isometric Advantage
The Isometric Advantage
Most of the time when people strength train they are focused on how much weight they should lift and how many sets and repetitions they should perform. While this impacts training adaptations related to strength, endurance, and power, I challenge you to think of one other variable – how long you should hold a position on tension. When your muscles are contracting to maintain a position without movement, this is called an isometric contraction. Here are 3 reasons why you should add isometrics to your training regimen:
Isometric exercises are under utilized
Isometric exercises, maintained contractions without movement, are under-rated and under-utilized in most training programs. When we hold a contraction for an extended period of time our brain sends signals to the working muscles to recruit more and more motor units. Motor units are composed of a motor nerve and all of the muscle fibers it innervates. When you squat, you do not fire all of the motor units in your quads, glutes, hamstrings, etc during every repetition. Your body is smart and moderates how many units are needed based on load, and varies this slightly with each repetition to help avoid fatigue and maximize strength output. Isometric exercises help us access a greater number of motor units through a process called summation. This, in turn, will enhance the variability of our muscle recruitment and allow us to access a greater degree of our inherent strength. Pain and injury will negatively impact motor unit recruitment and the primary means of reinstating optimal motor unit recruitment is progressive isometric training.

Own the position
Isometric exercises allow us to fully ‘own the position’ and therefore ‘own the movement ’. When you hold a bodyweight squat position for 30 seconds you have time to evaluate and feel your form / technique. Is your weight distributed equally between big toe / little toe / and heel (foot tripod)? Are your quads and glutes doing the majority of the work? Is your back and core stabilizing but not straining? Are your shoulders and neck position in line with your spine? It is more challenging to be aware of all of these variables when performing repetitions, and therefore there is significant value in performing isometric exercises, particularly for rehabilitation and learning proper technique. Once you have performed holds to ‘own the position’ you can transition to slow, controlled repetitions, trusting that your mechanics are spot on.
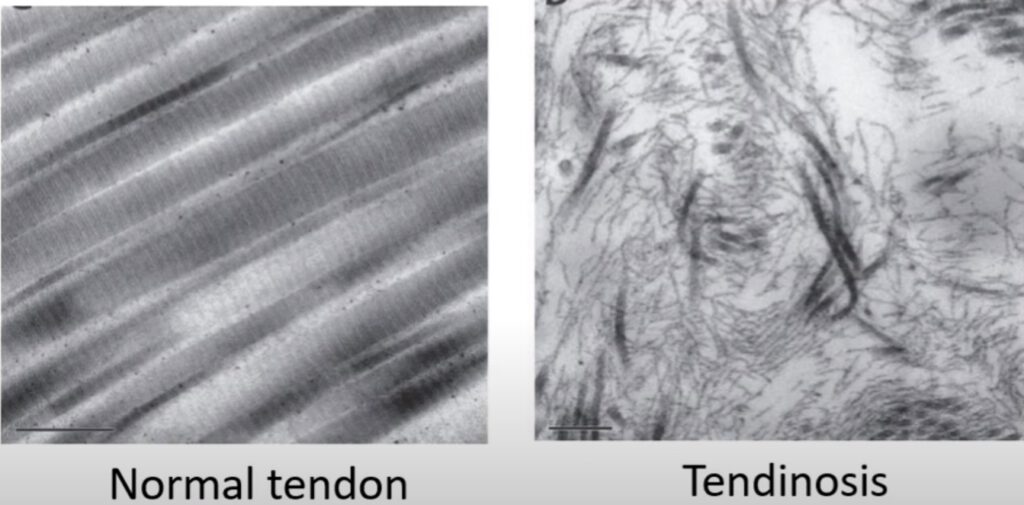
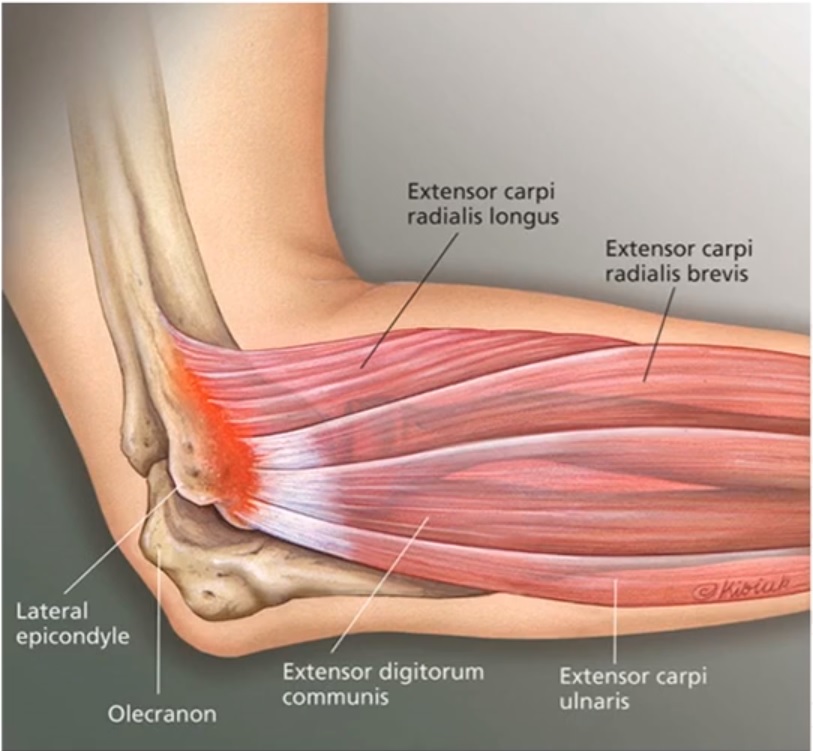
Decrease pain
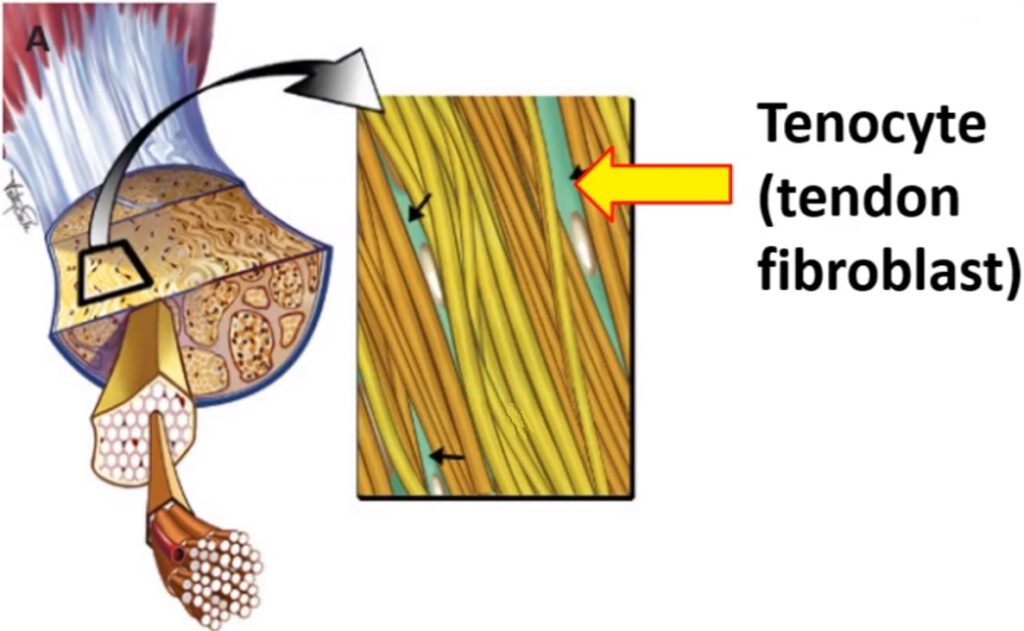
Isometric exercises will help decrease pain associated with tendon dysfunction. If you are suffering from tendinitis or tendinopathy you need to incorporate isometric holds into your rehab program. When using isometric exercises for tendon pain, start in the middle of a range (not end range) and hold the position for 30-60 seconds. Perform 3-5 repetitions. You can do this every day and progress the range and duration as you become more comfortable.
Ready to start? Try these foundational exercises to enhance upper and lower body strength:
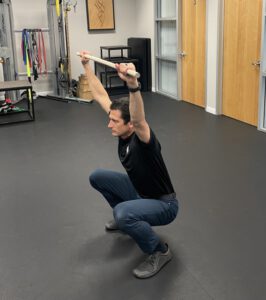
- Isometric bodyweight squat – Drop down into a squat position. Make sure your back is straight. Feel the weight in the middle of your feet – equal between big toe, little toe, and heel. Engage your legs in an exaggerated way (like you are trying to push the floor down an inch), so that your back can stay relaxed. Hold this position for 30 seconds to 1 minute.
Ready to start? Try these foundational exercises to enhance upper and lower body strength:
- Isometric bodyweight squat – Drop down into a squat position. Make sure your back is straight. Feel the weight in the middle of your feet – equal between big toe, little toe, and heel. Engage your legs in an exaggerated way (like you are trying to push the floor down an inch), so that your back can stay relaxed. Hold this position for 30 seconds to 1 minute.
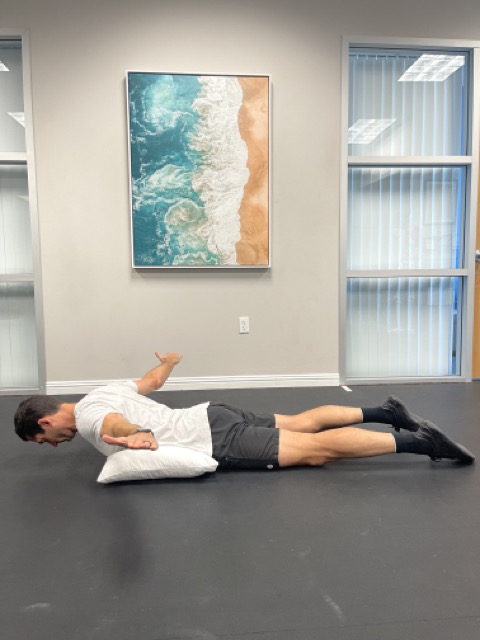
- Isometric scapula ‘T’ stabilization – lie on your stomach, supporting your low back with a pillow, and your head and neck with a towel. Lift your arms out to the side, pinching your shoulder blades together. Keep your elbows locked out. Don’t shrug your shoulders up towards your ears. Hold this position for 30 seconds to 1 minute.
If you’re ready to incorporate isometric holds into your routine or need guidance on how to safely implement them, please contact your local IPA Physio location for expert advice and personalized support. We’re here to help you achieve your fitness and rehabilitation goals!